In the high-precision world of orthopedic trauma surgery, the challenge of managing metaphyseal fractures remains a significant hurdle. The metaphysis is the transitional zone of a long bone, located between the dense, tubular diaphysis (shaft) and the articular epiphysis (the joint end). Because this region is composed of a thin outer shell of cortical bone and a complex internal network of cancellous bone, it is particularly susceptible to “shattering” or comminution during high-energy impacts.
The development of the Locking T-Fix T-Plate has provided surgeons with a sophisticated mechanical solution to these anatomical puzzles. By integrating the structural benefits of a contoured “T” shape with the advanced stability of locking screw technology, this implant has transformed the treatment protocols for fractures of the wrist, shoulder, and ankle.
The Mechanical Logic of the Locking T-Fix T-Plate
To appreciate the clinical utility of the Locking T-Fix T-Plate, one must first understand the shift from traditional compression plating to locking internal fixators. In a standard plating system, stability is achieved through friction. The screw pulls the plate tight against the bone, and the resulting friction prevents movement. However, in the metaphyseal region, the bone is often too soft or too fragmented to provide a solid foundation for this friction-based system.
The Locking T-Fix T-Plate functions as a “fixed-angle construct.” The head of the screw has threads that lock into the corresponding threads in the plate hole. This creates a bridge-like structure in which the plate and screws act as a single, rigid unit. This design ensures that fracture stability does not depend on the bone-to-plate interface but rather on the hardware’s internal strength. This is particularly vital in the metaphysis, where bone density may be compromised by age or injury.
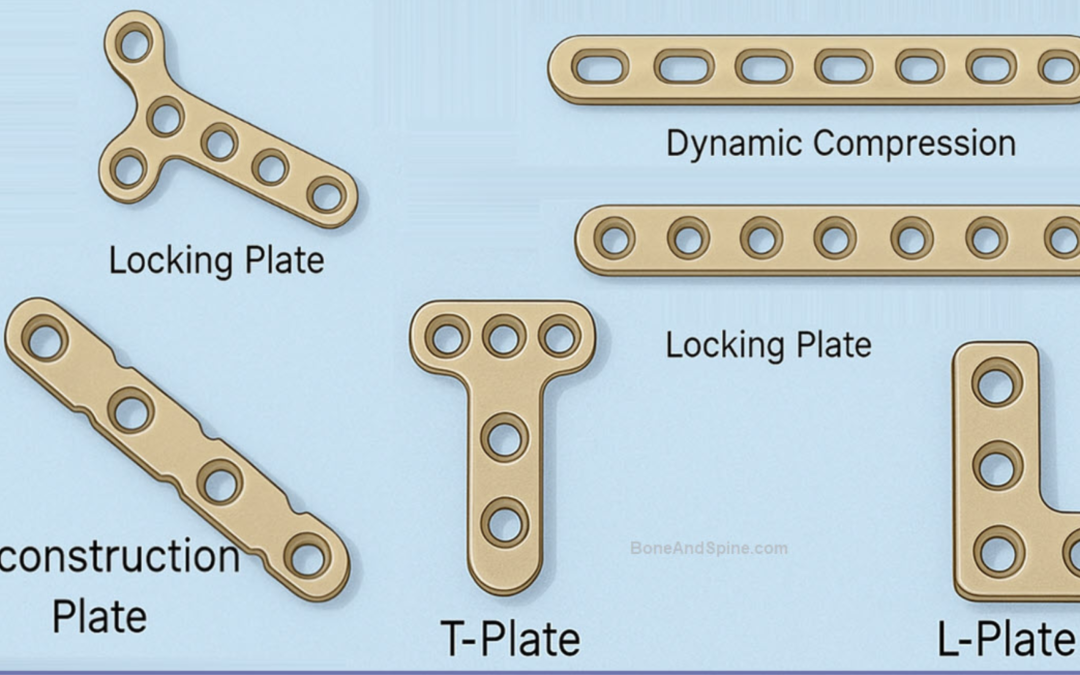
Strategic Design: The Power of the “T” Configuration
The “T” shape of the Locking T-Fix T-Plate is not arbitrary; it is a masterclass in anatomical engineering. The horizontal bar (the head of the T) is designed to sit across the widest part of the bone near the joint. This allows for the placement of multiple screws in a divergent or convergent pattern, which “rafts” or supports the joint surface from underneath.
The vertical portion (the shaft) extends down the bone, allowing for fixation into the stronger, cortical bone of the diaphysis. This dual-zone fixation allows the surgeon to anchor a fragmented joint end to a stable shaft, effectively “bridging” the zone of injury and allowing for early mobilisation.
Primary Indications: When is it the Best Choice?
Surgeons typically reach for a Locking T-Fix T-Plate in scenarios where traditional fixation methods are likely to fail. These specific clinical indications include:
1. Complex Distal Radius Fractures
The wrist is perhaps the most frequent site for this implant. When a fracture extends into the joint (intra-articular) or when the bone fragments are displaced toward the palm or the back of the hand, the T-design allows the surgeon to capture even the smallest fragments of the radial styloid or the ulnar notch.
2. Proximal Humerus Injuries
The head of the humerus (shoulder) often breaks into several pieces in elderly patients following a fall. Using a Locking T-Fix T-Plate allows for a “multi-planar” screw approach. By angling the locking screws in different directions through the T-head, the surgeon creates a “cage” of support that prevents the humeral head from collapsing or tilting into a malaligned position.
3. Management of Osteoporotic Bone
In patients with low bone mineral density, standard screws often “strip” the bone threads during insertion, leading to a loss of fixation. The locking mechanism of the Locking T-Fix T-Plate provides superior “pull-out strength.” Since the screws are locked to the plate, they cannot toggle or back out, even if the bone surrounding them is weak.
4. Corrective Osteotomies
Beyond trauma, these plates are used in elective surgeries where a bone must be cut and repositioned to correct a deformity. The T-shape provides the necessary stability to hold the newly aligned bone in place while the gap fills with new bone growth.
Advanced Surgical Techniques and Principles
Successful implementation of the Locking T-Fix T-Plate requires a strict adherence to modern surgical principles. It is not enough to simply “bolt” the plate to the bone; the biological environment must be respected.
Anatomical Reduction and Alignment
Because locking plates are extremely rigid, they do not “self-correct” the bone as the screws are tightened. In non-locking systems, the plate can sometimes pull the bone into alignment. With a Locking T-Fix T-Plate, the surgeon must achieve a perfect or “near-perfect” reduction of the bone fragments using temporary pins or clamps before the first locking screw is inserted. If the bone is locked in a crooked position, it will heal in that position.
Preservation of the Periosteum
One of the greatest biological advantages of this plate is that it does not need to be pressed flush against the bone surface to be stable. This “stand-off” capability preserves the periosteum—the thin layer of vascular tissue that covers the bone. By maintaining the blood supply to the fracture site, the Locking T-Fix T-Plate promotes faster “callus” formation and reduces the risk of non-union (where the bone fails to heal).
The Hybrid Technique
Experienced surgeons often use a “hybrid” approach. They may use a standard cortical screw in the shaft to pull the bone toward the plate and achieve initial alignment, followed by a series of locking screws in the T-head to finalize the rigid fixation. This combines the best of both worlds: the “draw” of traditional screws and the “locked-in” security of modern technology.
Conclusion: A New Standard for Recovery
The evolution of the Locking T-Fix T-Plate has fundamentally changed the recovery trajectory for patients with metaphyseal injuries. In the past, these fractures often required long periods of immobilization in heavy casts, leading to permanent joint stiffness and muscle atrophy.
Today, the absolute stability provided by the Locking T-Fix T-Plate allows for “functional aftercare.” In many cases, patients can begin gentle range-of-motion exercises within days of surgery. By allowing for early movement while ensuring the bone fragments remain perfectly aligned, this implant helps patients regain their independence and return to their daily activities with a significantly lower risk of long-term disability. As material science continues to improve, these plates will only become lower in profile and more “anatomically perfect,” further cementing their role as an indispensable tool in the orthopedic arsenal.