Femoral fractures are among the most debilitating orthopedic injuries encountered in emergency medicine. Due to the high-energy trauma typically required to break the femur—the strongest bone in the human body—these injuries are often accompanied by significant soft tissue damage, internal bleeding, and intense muscle spasms. In the acute phase of treatment, stabilizing the limb is not just about bone alignment; it is a critical step in pain management and preventing further vascular or neurological complications.
Among the various stabilization techniques available, skeletal traction remains a cornerstone of emergency orthopedic care. Specifically, the use of Steinmann Pin Traction provides a reliable, time-tested method for maintaining limb length and alignment before definitive surgical intervention can take place.
The Role of Skeletal Traction in Acute Trauma
When a femoral shaft fracture occurs, the powerful muscles of the thigh—the quadriceps and hamstrings—contract instinctively. This contraction causes the fractured bone ends to overlap, leading to significant shortening of the limb, intense pain, and potential damage to the femoral artery or sciatic nerve.
While skin traction (using adhesive straps or boots) can be used for minor stabilization, it is often insufficient for adult femoral fractures. The force required to overcome thigh muscle spasms is usually greater than what the skin can tolerate without breaking down. This is where skeletal traction becomes essential. By inserting a high-grade stainless steel or titanium pin directly through the bone, surgeons can apply the necessary weight to counteract muscle pull and stabilize the fracture site effectively.
In modern surgical environments, utilizing high-quality instruments from trusted providers like Ortho Care ensures that the hardware used—from the pins to the stirrups—meets the rigorous demands of trauma surgery.
Understanding the Steinmann Pin
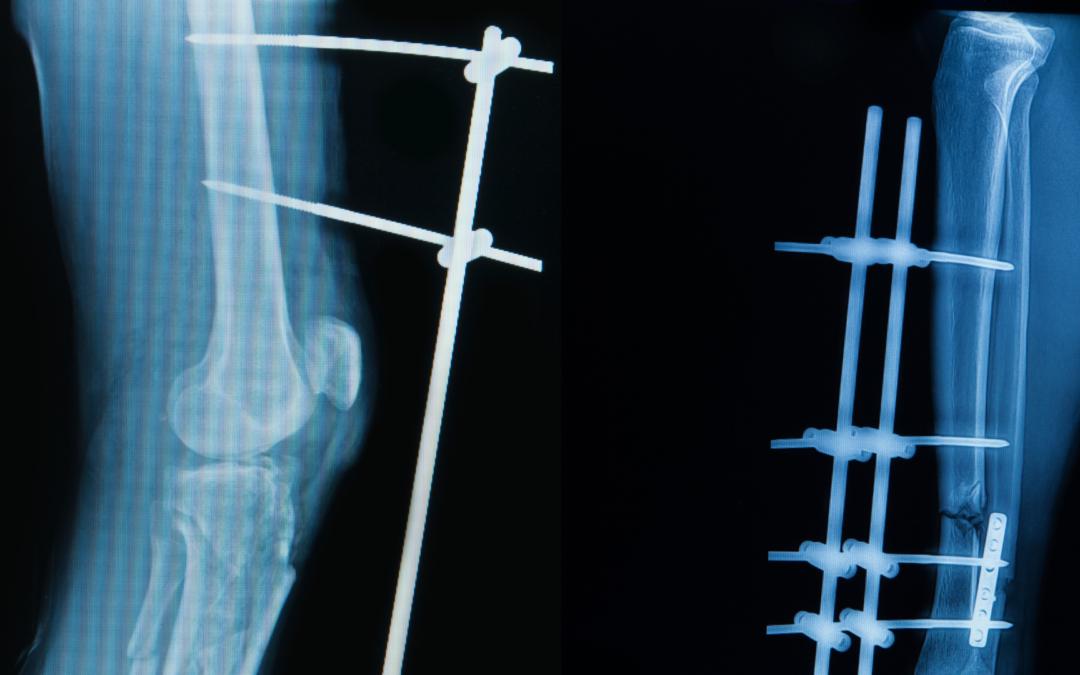
The Steinmann pin is a rigid, cylindrical metal rod used frequently in orthopedic surgery. Available in various diameters—typically ranging from 3.0mm to 5.0mm for adult femoral applications—these pins are designed to be driven through the bone to act as an anchor for external weights.
In the context of femoral fractures, the pin is most commonly placed in the proximal tibia (just below the knee) or the distal femur (just above the knee). The choice of site depends on the location of the fracture and the planned definitive surgery. For most mid-shaft femoral fractures, a proximal tibial pin is preferred as it keeps the surgical field for the future femoral nail clear of potential pin-site infections.
The Procedure: Precision in the Emergency Room
The application of skeletal traction is a minor surgical procedure often performed at the bedside under local anesthesia or conscious sedation. The process requires a meticulous approach to avoid damaging vital structures.
- Site Selection and Preparation: The area is cleaned with antiseptic solution, and the entry and exit points are infiltrated with local anesthetic.
- Pin Insertion: Using a manual or power drill, the pin is inserted through the bone. In the case of proximal tibial traction, the pin is placed approximately 2cm posterior to the tibial tuberosity to avoid the growth plate (in younger patients) and the joint capsule.
- Traction Application: Once the pin is secure, a “Bohler stirrup” is attached to the ends of the pin. A cord is then run from the stirrup over a pulley system at the foot of the bed, where weights are applied. Generally, the weight used is approximately 10% to 15% of the patient’s body weight.
Femoral Nail: The Definitive Solution
While Steinmann Pin Traction is an excellent temporary measure, it is rarely the final treatment for an adult femoral fracture. Modern orthopedic standards favor early internal fixation to allow for faster mobilization and to reduce the risks associated with prolonged bed rest, such as deep vein thrombosis (DVT) or pneumonia.
The “gold standard” for treating femoral shaft fractures is the intramedullary Femoral Nail. This procedure involves inserting a metal rod into the hollow medullary canal of the femur. The nail is locked into place with bolts at both ends, providing internal stability that allows the patient to begin weight-bearing exercises much sooner than traditional traction would allow.
The period spent in skeletal traction is vital for “soft tissue rest.” By reducing the fracture and maintaining alignment, the traction helps the swelling subside and prevents the muscles from becoming permanently shortened, which makes the eventual insertion of the nail significantly easier and safer for the surgeon.
Risks and Maintenance
Managing a patient in skeletal traction requires vigilant nursing care. The most common complication is a pin-site infection. To prevent this, the areas where the pin exits the skin must be kept clean and dry, often using saline-soaked gauze.
Furthermore, clinicians must monitor for:
- Neurovascular Status: Regularly checking pulses, sensation, and motor function in the foot to ensure the traction isn’t compressing nerves or vessels.
- Over-distraction: Applying too much weight can pull the bone ends too far apart, which may hinder the natural healing process (non-union).
Conclusion
In the high-pressure environment of emergency orthopedics, the ability to quickly and effectively stabilize a femoral fracture is paramount. The application of skeletal traction using a Steinmann pin serves as a vital bridge in the patient’s journey from injury to recovery. By neutralizing muscle spasms and restoring limb length, it provides immediate pain relief and prepares the biological environment for successful definitive fixation.
Relying on precision-engineered components from Ortho Care during these initial stages ensures that the foundation for the patient’s recovery is as stable as possible, ultimately leading to better outcomes when transitioning to definitive femoral nailing.